We found that four published gene sets for hypoxia that have been validated to predict outcome in head and neck cancer had little overlap in terms of included genes. Nevertheless, they classified patients in an almost identical manner, indicating that they all reflect the same underlying process. This underlying biological process correlated with chronic, and not acute, in vitro hypoxia. While the validated prognostic profiles showed no resemblance to in vitro early hypoxia response, this acute response (and not the chronic response profile) was a significant predictor of local recurrence in 91 HNSCC patients treated with chemoradiotherapy.
Same classification, different gene sets
The phenomenon that signatures consisting of different genes can describe the same process, has been reported by Roepman et al [41]. They showed that multiple robust signatures to predict the presence of lymph nodes in head and neck cancer could be created from a larger group of predictive genes, which were not all needed to form an accurate predictor. Given the fact that over 4,000 genes are hypoxia-regulated, it seems reasonable to assume that multiple robust, but entirely different, hypoxia signatures can be assembled [42].
Acute and chronic hypoxia
The terms acute and chronic hypoxia are obviously simplified terms to describe a spectrum of hypoxic cells in a tumor [43]. While an absolute distinction between the two cannot be made, many suggestions for the separate origin, measurement and treatment of the two entities have been published [44, 45, 46, 47].
Janssen et al. employed various staining protocols to study acute and chronic hypoxia in head and neck tumors [45]. They showed that tumors contained on average 15% acute hypoxic (proliferating cells around temporarily non-perfused vessels) and around 30% chronic hypoxic areas (cells at a large distance from blood vessels). The two types of areas showed no overlap. This was also reflected in gene expression profiles of cells. Cells that had been under hypoxia for a short time, showed a very different gene expression as compared to cells that were hypoxic for longer periods of time [37]. As described by Lendahl et al. in a colon carcinoma cell line, 4,047 genes were hypoxia-regulated, of which only 52 were specific for acute (1 or 2 hour) hypoxia response, 144 genes were up- or downregulated by both acute and chronic (24 hour) hypoxia, whereas the majority of the genes (4,005) were chronic hypoxia specific [42].
Nonetheless, all creators of hypoxia signatures have tried to generate one signature for ‘general hypoxia’. The fact that these signatures correlated with in vitro chronic hypoxia could simply be due to the large excess of genes regulated by chronic hypoxia [42], but also to the methods used for the generation of the signature. For the Toustrup et al. profile an explanation could be that they correlated genes with eppendorf probe measurements. If indeed on average twice the amount of chronic hypoxic areas is present, as reported by Janssen et al, this could lead to a stronger correlation with chronic hypoxia genes. Winter, Buffa and Eustace et al. started with 10 hypoxia ‘seed genes’ to develop their signatures. In our data, these 10 genes were not correlated with in vitro acute hypoxia and most showed some correlation to late in vitro hypoxia (Table 5.3).
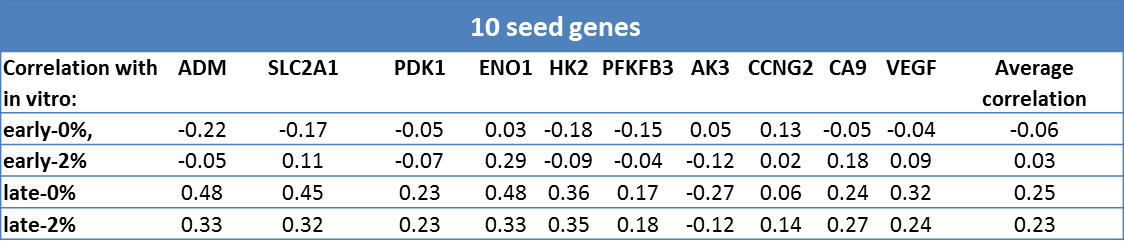
Table 5.3. Correlation of 10 ‘seed genes’ with in vitro acute and chronic hypoxia profiles.
Acute hypoxia and prognosis
The importance of acute hypoxia has been recognized for decades [48]. For example, Chan et al showed that a human lung squamous cell carcinoma cell line (H1299) became more radioresistant under acute hypoxia than under chronic hypoxia, with respective oxygen enhancement ratios of 1.96 and 1.37 [49]. Unfortunately, conclusive data on the separate and combined prognostic effects of acute and chronic hypoxia in head and neck tumors are lacking. This might be due to the fact that it is difficult to measure both types of hypoxia with immunohistochemistry.
Cutoff and effect size of hypoxia status
Using the median expression as a cutoff to create two groups, we found that patients with high acute or chronic hypoxia expression, had a 3.1 or 1.8 times higher risk of local recurrence, respectively. Although the latter was not significant, possibly due to the number of patients, the effect size appears comparable to previously reported hazard ratios for chronic hypoxia. Toustrup et al. found that the risk of locoregional recurrence was 1.85 times higher for “more hypoxic” tumors compared to “less hypoxic” tumors. Eustace et al. reported in their series of larynx carcinoma patients that the “more hypoxic” tumors receiving accelerated radiotherapy had a 5-year recurrence rate of 19%, while the patients with “less hypoxic” tumors had a recurrence rate of 9%. Winter et al. also reported recurrence-free survival, but compared the highest quartile to the rest of the patients. Using this method, the HR was 3.6 in a univariate analysis and 2 in a multivariate model. Buffa et al. reported a HR of 6.25, though the confidence interval (0.83-47.2) indicated a high level of uncertainty.
Hence for chronic hypoxia gene expression signatures, the general deduction is that more hypoxic tumors are approximately twice as likely to recur than the less hypoxic tumors. This effect could be underestimated due to a division of two hypoxia groups according to the median. Furthermore, acute hypoxia has not been studied in these series, but might well be more predictive than chronic hypoxia.
Conclusion
Different sets of genes can be used interchangeably to study the extent of hypoxia-driven gene expression in head and neck cancer. Although they scarcely contain overlapping genes, published gene sets for hypoxia that have been proven to be prognostic in head and neck cancer classify patients into the same riskgroups. These published sets all correlate with chronic and not with acute in vitro hypoxia-induced gene expression profiles. However, the acute hypoxia profile correlates better with the risk of recurrence after chemoradiotherapy in our series. Acute hypoxia gene expression should therefore be incorporated into existing hypoxia-based prediction models.